
Before I begin, I want you to know that I am okay. This post includes a traumatic event that is important for me to write about and process.
I’m writing this from my hospital room, sitting by the window. The sky is dreary, and I can’t wait for spring to feel like spring. You may ask, “Didn’t you already leave the hospital?” Yes—over three weeks ago—but I can’t seem to stay away.
This past Tuesday, I was home putting soup in the microwave, and went to plug in my phone since the battery was almost dead. When I stood up, I started to feel lightheaded and faint. Unsure if I would pass out, I sat down quickly and checked my blood pressure and pulse. My pulse was 164 (high for resting), and my blood pressure was normal. A few minutes later, my blood pressure was high and my pulse had normalized. I’ve experienced this feeling before, usually when I stand up too fast, but given the fact that I had heart surgery almost five weeks to the day, I called the hospital to page the on-call doctor from my surgical team.
The fainting feeling dissipated, but I continued to have ringing in my ears and pulsing in my head. Ten minutes later, as I waited for the call from the doctor, I started feeling faint again. This was much worse. I felt forced to lie down since I was on the verge of actually passing out. Fortunately, the feeling again went away. I knew that since this happened at rest, whatever was going on wasn’t simply due to standing up too fast. Something was wrong, and I needed help.
I called 911…
On the phone with the dispatcher, I explained my symptoms and that I had a very extensive heart surgery recently. The doors weren’t unlocked, so he encouraged me to slowly get to the door. Fortunately, the event didn’t happen again as I stood up. Unfortunately, the paramedics and fire department went to the wrong door – just my luck!
EMS checked my vitals and made sure I was stable enough to be transported. Given the cardiac issues, they called for a specialized ambulance team, and they loaded me into the back. The paramedics hooked me up to all the wires, asked me a bunch of pertinent questions, and took my vitals. Five minutes later, I started feeling faint again, but this was worse than the previous two combined. My heart started to race, and the paramedics quickly shifted gears from a relaxed approach to a controlled, but urgent reaction. I was instructed to bear down as much as I could to do a valsalva maneuver. The paramedics started moving faster. I could feel my heart racing as I became increasingly faint while trying to take deep breaths and bear down. That’s when I saw them start to put defibrillator pads on my chest.
When I think of a defibrillator, I think of someone in cardiac arrest. As an EMT, that was the only reason I had put defibrillator pads on a patient in case they were at risk of their heart stopping. While I was experiencing a bunch of symptoms, I assumed that it would dissipate just like the past two events. I started to panic and asked the paramedic if this was necessary, but he was adamant about the urgency of the situation. He told me that my pulse was 240 and my systolic blood pressure was 60. I sometimes wish I was ignorant to medical jargon, but from my experience, I knew how serious this was.
One of the paramedics questioned if they should administer any sedative medications, but they came to the conclusion that there was no time. They told me that they needed to shock me, and it was going to “feel like a big kick.” I started to hear the defibrillator charge. Then I heard the words from CPR and EMT training, “I’m clear, you’re clear, we’re all clear.” Then they pressed the button.
The shock was worse than a big kick. It was like a sword stabbing into my torso combined with sharp needle-like electricity coursing throughout my body. It wasn’t quick — it lasted a few seconds. And I can tell you that the medical dramas aren’t that much of an exaggeration as my body tensed up, lifting partly off the stretcher.
After the pain improved, and I was able to orient myself, I realized that all of my symptoms were getting better. I was feeling closer to normal, and the paramedic assured me that my pulse and blood pressure were also back at a good range.
I took deep breaths as they rushed me to MGH (where I had my heart surgery). The paramedic stayed on high alert in case I became unstable again. He gave me one minute to call Chris. I reached Chris on the phone, and I was overwhelmed, quickly telling him that I was in an ambulance and just got shocked. I said, “Come to MGH, and call my mom.” The paramedic urged me to hang up, so I had to end the conversation abruptly. I can’t imagine what it was like for Chris to get that phone call.
I continued to ask the paramedic for my vitals as I was nervous my condition would get worse again. We finally arrived to the MGH emergency room. The silver lining of getting a shock is you get to skip the whole ER line. Controlled chaos happened around me as IV lines were put in, images were taken, and countless doctors and nurses asked me questions. I remained stable as Chris arrived at the ER, and we waited to get some answers.
I was in emotional shock, compartmentalizing my feelings in order to focus on communicating what had happened as well as digesting all of what the doctors were saying. My immediate worry was that something went wrong with either my valves or ascending aorta from the surgery just five weeks prior. They performed an ultrasound, which showed no fluid, making a surgical leakage less likely. Later on, they also took a chest x-ray as well as an echocardiogram to rule out any structural issues. Fortunately, the surgical team was reassured that the heart looked normal for five weeks post-operation.
So, if it wasn’t a complication from the Ross Procedure, what happened? The cardiology team came in to explain that I experienced either a Supraventricular Tachycardia (SVT) or a Ventricular Tachycardia (VT). These are two types of arrhythmia (abnormal heart rhythms).
A SVT is when the heartbeat is too fast and starts in the heart’s upper chambers (atrium). It is relatively benign and doesn’t usually require treatment.
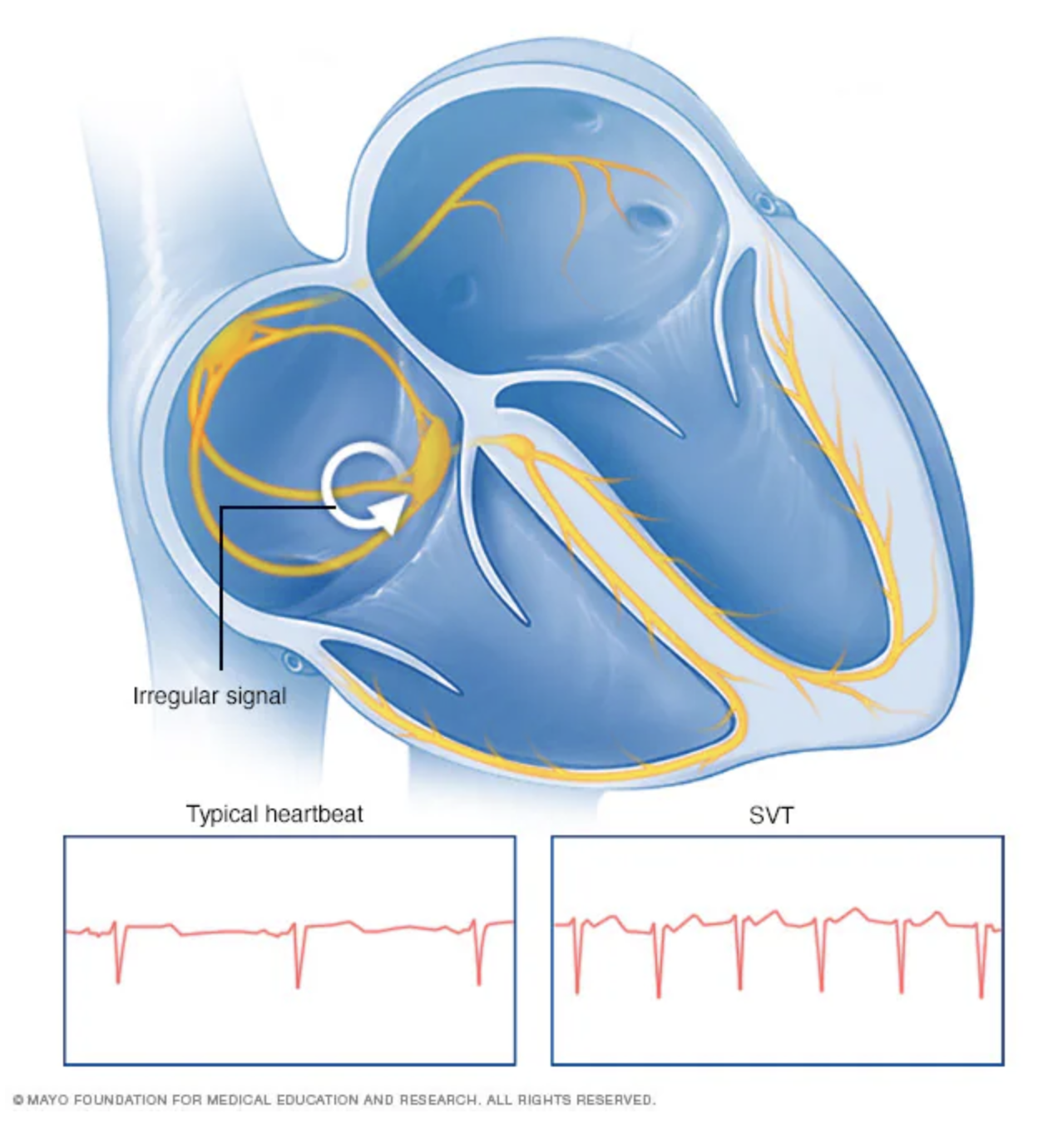
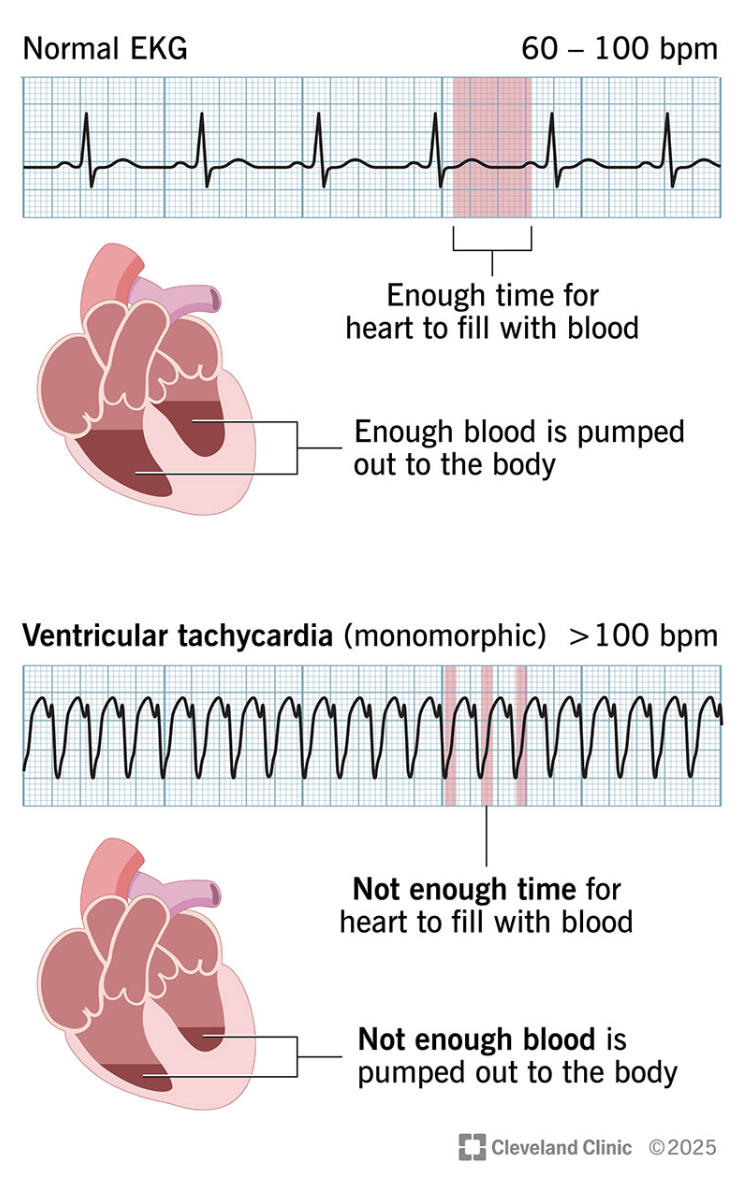
A VT is a fast heart rate that starts in the heart’s two lower chambers (ventricles). Unlike SVT, VT can be life-threatening.
I was fortunate that the paramedics were able to get an EKG right when I was having the event so the doctors could diagnose between SVT or VT. Unfortunately, as always, mine was a bit more complicated. I found out I had a preexisting Right Bundle Branch Block (RBBB), which is when the electrical signal to the right ventricle (bottom) of my heart is delayed. While the ventricles are supposed to beat at the same time, the RBBB causes my right ventricle to contract later than the left.
So, why does this matter? The spacing between part of the heartbeat shown on the EKG is one way they distinguish between SVT and VT, where VT is wider. Due to the RBBB, my normal rhythm is wider than most people’s. The doctors needed to determine whether the spacing was because of the RBBB and thus SVT, or if it was VT.
Despite having the cardiology, cardiac surgery, and neuro-oncology teams consulting with one another, they needed to bring in the specialists of arrhythmias, the electrophysiologists. These are the Jedis of the heart’s electrical system. They see things in EKGs that others cannot.
Each team met with me in the ER. The plan was to admit me so they could discuss as a group the next day about what they think is happening, and what the next steps should be.
Even with all of these teams discussing my case, there was still uncertainty about whether it was a SVT or a VT. The first thought was that I had a SVT and could go home with an external heart monitor. The plan shifted towards a more conservative approach in case it happened to be VT. They started me on a medication called Sotalol since it acts as an anti-arrhythmic medication for not only VT, but also SVT. After further conversations between the electrophysiologists, they began to feel more confident that I had a VT event. With that conclusion, they recommended the medication as well as a Subcutaneous Implantable Cardioverter-Defibrillator (ICD)
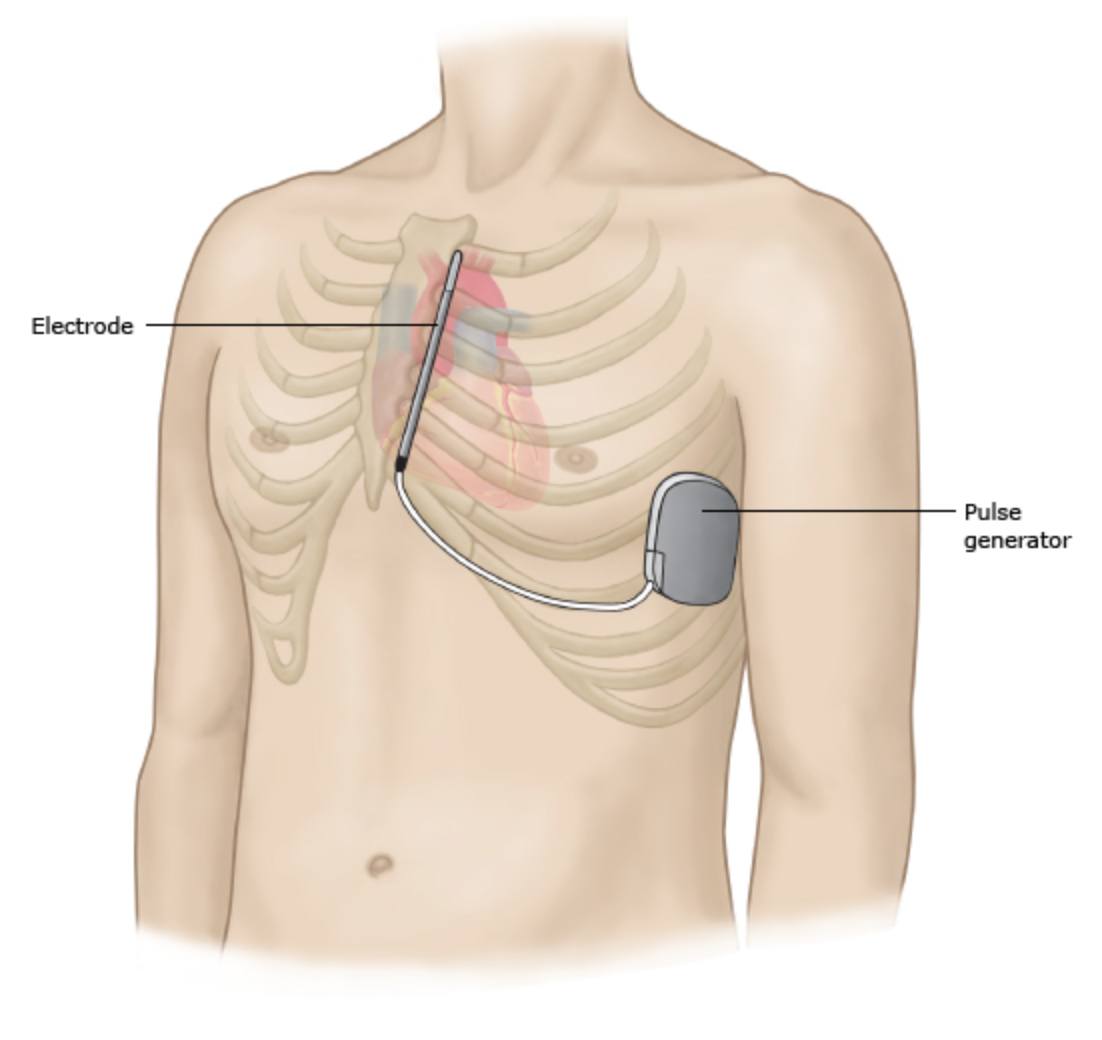
An ICD is implanted in the body to shock the heart if there is a dangerous abnormal heart rhythm (similar to what the paramedics did on me). While most ICD wires are placed through the vasculature and into the heart, due to my age, as well as my recent heart surgery, it was determined that a subcutaneous version was better. As you can see below, the generator for the ICD is placed just under the armpit in between two muscles, and the electrode is implanted vertically along the breast bone. I was educated thoroughly on this, but I questioned whether the plan would shift again, or if this was even the right approach since we still didn’t definitively determine whether it was SVT or VT.
It was unnerving having the plans shift in real time, but it was also reassuring that the doctors were actively and methodically communicating with one another. In medicine, each doctor may have a different opinion, and speciality teams might have different approaches. This is ultimately a good thing because the act of questioning and challenging others’ opinions often results in a more well-thought-out solution.
Despite having all of these medical teams working together to discuss my case, I still wanted to get another perspective. With all the procedures I have had in my life, I usually search for a second opinion at a different institution. I recognize that my ability to do this is a privilege most people do not have access to. I’m lucky that my primary care physician had a close connection with an electrophysiologist at Brigham and Women’s Hospital. His recommendation was to do an electrophysiology study first before taking the step to implant a defibrillator.
An electrophysiology study (EP Study) uses catheters inserted into the heart via veins in the groin to find out where abnormal heartbeats are coming from. In the image below, the orange and blue wires stimulates the atrium whereas the green wire stimulates the ventricle.
The benefit of an EP Study is that it can provide a clearer picture of what type of abnormal heart rhythm exists. In my case, they were avoiding it because from the EKG they were pretty sure that I had a VT, and even in the chance that it was a SVT, the treatment for the VT would be protective. Additionally, it is an invasive procedure on a normal person, let alone a five-week-out Ross Procedure patient.
The EP from Brigham and the EP from MGH talked with one another. I have heard from many patients that they are often hesitant to ask for a second opinion as to not offend the doctor. In my experience, the doctor usually doesn’t mind, and if they do mind, they might not be the right doctor. For me, I do whatever I can to feel as confident as possible in the treatment plan.
After the EPs discussed my case, they agreed that doing an EP study first was the best next step to see if they can reproduce my EKG (heart rhythm pattern) from the ambulance by trying to induce a SVT. If it ended up being a VT, then the defibrillator would be implanted.
The next day, I was brought down to the operating area. Similar to my heart surgery (and my brain surgeries), I told Chris and my mom, “see you soon.” Just a few minutes before being brought down, I was informed that a different physician than the one I was seeing was going to do the procedure. I was caught off guard. For me, I usually build trust with a physician by developing a relationship in person through both medical and everyday conversations. I had no idea who this other doctor was. Noticing my hesitancy, the nurse gave me an option to switch, but she was confident in this physician’s abilities, which put me a bit at ease.
When I met the doctor, I immediately knew I could place my trust in her for the procedure. She had a calm demeanor, didn’t rush our interaction, and answered my questions thoughtfully. After she went through the whole plan, they brought me into the operating room to prep me as we played Andy Grammar on the speakers to set the mood.
I was lightly sedated, but still awake, as they guided the catheters to my heart. During the EP study, I needed to be awake so that my heart would be in a normal state to test it. I wasn’t too stressed as I am all too familiar with being awake during a procedure. I was awake during my 2018 brain surgery, which to say the least, was a tad more extensive.
As they worked to trigger a SVT, I could feel my heart getting fast and then slowing down. Quickening again, and then slowing down. At times it would skip some beats, which was distressing, but they kept me calm with the sedation. One of the doctors stood by my side, guiding the wires and providing the shocks, while the other doctor I met earlier was in the control room assessing the rhythms in real time. They all wore headsets talking to each other as they searched to replicate my arrhythmia.
The study finished and the doctor came next to me. She explained that despite everything they were doing, they could not replicate my arrhythmia by stimulating the areas of the heart that would indicate a SVT. This meant that they were 100% confident that what I experienced was a ventricular tachycardia (VT). I asked if they tried to replicate the VT, and they did provide some stimulation, but given that they could not replicate a SVT as well as the risks of inducing a VT on my heart post-surgery, they were content with the findings. While my recent heart surgery may have triggered the episodes, they believed I have lived with the arrhythmia for a long time, so a durable, protective approach was necessary. They needed to implant a defibrillator.
The next thing I knew, the nurses were moving all around me deconstructing the EP study setup, and getting the defibrillator process prepped. They put me on an oxygen mask as I drifted to sleep.
I woke up in the recovery unit sore under my left arm and upper chest. I was now officially bionic! When they brought me back to my room, Chris was there to greet me. While I was still incredibly fatigued and nauseous, I could sense our shared emotions: relieved, grateful, and traumatized.
The confirmation of ventricular tachycardia put into perspective the reality of my episodes on Tuesday. During the second episode, I was nearly at the point of passing out. If that were to have happened, this could have been fatal because I would have had no way to get help. I have been through a lot in my life, but this is the first time that I know and can vividly remember how close to the edge I was.
The silver lining of having this happen now, is that it didn’t happen when I was somewhere I couldn’t get help like on a hike or a boat. Part of me is a bit relieved that it was found to be VT because I now have the defibrillator as a safety net if anything were to happen again. While a SVT would of course be easier to live with, I would always wonder, “what if there is a chance I would have a VT. Would I be okay?”
Now I know that I will be okay.
I preemptively scheduled a therapy appointment next week because I know once I get home the emotions will spill out. The memory of the ambulance ride will stick with me for a long time. The memory of having the stroke-like symptoms after my heart surgery will stay with me too. All of these “traumas” have been accumulating, and I need to make sure I don’t bottle them up.
Like all the times before, it is Chris, my mom, family, friends, my PCP, and the doctors and nurses who have helped me get through this. Today, I will finally get discharged and I hope I do not need to come back to MGH inpatient for a very long time.
In my writings about my journey with brain cancer, I have talked about how it has shaped who I am and what I value. As I leave the hospital today, and transition from survivor mode to recovery, I’ll learn more about how this experience has affected me. It is not hyperbole to say this has put life into perspective. It’s a different kind of perspective than the one shaped by the past 20+ years of my medical journey. Knowing how close I was to things being very different is the most tangible reminder I’ve had of how fragile life is. It is a reminder to hold those I love close and to not take for granted this one beautiful life we have.
It’s about time for my heart to stop being jealous of all the attention I give to my brain. They both need to cooperate because I’m ready to move forward with living life, getting married, and becoming a father.
With love,
Jeremy

Keep healing our brave Jeremy. We are always rooting for you and appreciate your updates. My best to your mom.
Love, Lauren, Michael and Lindsay Corkin
LikeLike
Thanks Lauren 🙂
LikeLike
I think you are the bravest person I know. And your messages to your community of friends, and acquaintances are so valuable. I was just a TA in Brian Newmark’s room at Wayland High, but have thought over the years how extraordinary you are. You have all my support, for what that’s worth.Barbara Smith
LikeLike
Thanks Barbara. Means a lot. 🙂
LikeLike
Dear Jeremy, I learn so much from you. Not just the incredible details of your challenging medical moments, but the approach to living that you share. Thank you for bringing us along on your journey and sharing so openly and vividly. It certainly keeps each of our lives in perspective. As always I wish you all good moments going forward and much joy and happiness as a married man and potential father! With love,
Nancy (DiPerna) Tharler
LikeLike
Thank you Nancy 🙂
LikeLike
Thank you so much for sharing this experience. Wishing you health, love, and happiness always.
LikeLike
Thank you Stephanie
LikeLike
Wow, Jeremy! Harrowing(!) is the mot juste! I am so glad you came through this experience with a great and positive attitude.
All my best to you and Chris.
-Guy
LikeLike
Thank you Guy! All my best to you as well.
LikeLike