
***Some of you subscribed to my blog may be receiving this as an email for the first time since my previous post did not send out an automated notification. To understand the following, I would recommend reading my latest post When the can doesn’t land as far as you hoped – another recurrence***
Warning: This post is long! This is not the usual post where I dive into the emotional aspects of my experience. Rather, this is a pretty cut and dry description of my three weeks of meetings and calls to develop a treatment plan. During my 2014 recurrence, I wrote a similar (…yet less detailed) post about treatment decisions. I received a lot of messages from patients and family members of patients who found that post helpful. This is for that audience. My hope is that this very detailed explanation of my treatment meetings may shed some light on how much information is involved in informing a treatment plan. While I share a lot of detail, I want to note that this is my experience. Every individual’s situation and decisions will be unique to them.
I did not expect how helpful it would be to rewrite all of this from my notes. As I transitioned back to school in Berkeley, I developed an elevator speech to simplify this information for others, and unintentionally, for myself. Writing this post reminded me how much information went into my treatment decisions, what is known, and the extent of what is still unknown. Given this, I now feel like I can go into the next steps of my treatment with my eyes open.
To make this post digestible to various audiences, I provided an outline below. At the bottom of each section is a bulleted summary. If you simply want to know my treatment plan, you can scroll to the section, “Summary of Treatment Plan.” Additionally, for any patients reading this, I provided some tips at the very bottom of this post based on insights I’ve gained from having gone through this extensive process. If you have any questions, feel free to contact me.
As a fair warning, writing while drowsy from seizure meds and keeping up with medical school is difficult, so I apologize in advance for any poor writing! 🙂
To summarize: I will have an awake, brain mapping surgical biopsy and resection on May 22nd at UCSF. The following is what led to that decision:
Outline:
- UCSF Tumor Board Call
- Meeting with UCSF Neurosurgeon
- Meeting with MGH Neurosurgeon
- Meeting with Dr. Wen (a.k.a. Yoda) at Dana Farber
- Debrief with my family and PCP
- Clarification calls with UCSF Surgeon and Dr. Wen
- Summary of Treatment Plan
- Final Tips for Patients
UCSF Tumor Board Call (36min)
When dealing with cancer there are always significant dates that you mark on your calendar. Dates that you can’t get out of your head. You try your hardest to focus on the present and what you need to do, but as you get closer to the date, time slows down, and your chest tightens as the day arrives. In my last post, that date was March 10th. The day I had my MRI and was diagnosed with a recurrence. The next date was Thursday, March 15th. The day of UCSF’s tumor board meeting when a group of experts would discuss my case and come to a decision on what they as a UCSF team would recommend for treatment.
My neurooncologist at UCSF said she would call me after the meeting. Throughout the day in class I checked my phone obsessively, making sure I always had signal…ready to access my notebook…ready for yet another life-changing conversation to disrupt the normalcy of my everyday life.
The hours ticked by, and no call, no emails, no voicemails. I finished up a meeting at my program’s office suite regarding my master’s thesis and whether or not I could continue my project given my medical situation. We wrapped up our meeting, and as I walked towards the restroom, about to head home, I felt my pocket vibrate. My heart raced. I picked up the phone, and despite knowing who it was on the other line, I coyly answer, “hello.”
I asked my doctor to give me a moment to find a place to talk. My faculty and most of my classmates already knew about my medical situation, but this wasn’t a conversation I could have in a hallway. I needed a private space to feel comfortable asking difficult questions.
I pulled out my notebook and as I prepared to scramble down a bunch of notes, I wrote down one word: “Surgery.” Just like our meeting a few days prior, I was still confused how surgery could be an option since in 2014 my tumor was considered inoperable. My doctor said she would set up a meeting with the neurosurgeon, but explained that while a full resection is still out of the question given the location of the tumor bordering/within the motor strip, a partial resection of the area growing into the resection cavity may still be possible. Not a total resection, but partial.
She continued to share that the UCSF team was certain the changes seen on the scans could not be explained away by variations in MRI technique. Generally, they classify tumor progression as equal to or greater than 25% change in growth. Compared to my scan last August, there has been greater than 25% change. Since my scan in January, there has been a small change, but not up to 25%, so they do not clinically classify it as progression. This nuance is what makes slow-growing oligodendrogliomas so diagnostically challenging. It’s like the frog in a boiling pot. If the frog stays in the pot, comparing the temperature to the moment before, it doesn’t notice the change. However, if the frog is thrown straight into boiling water, it jumps out! The standard for comparing MRIs is to use the latest scan. For my type of tumor if we always use the latest scan then you would rarely see 25% change (you don’t notice the temperature changing). You need to look back at scans from quite a while back (comparing cold to boiling water). But when is enough growth enough? When do we need to act? When do I as a patient get told that my tumor has recurred? In reality, my tumor has never stopped growing. If we had looked far enough back, we probably would have seen significant change. So should I as a patient be told only when my tumor reaches the 25% benchmark, or should I know before then? These are questions I often think about and relate to my belief that patients should be partners in their care. Regardless, given the extent of growth since August, the UCSF tumor board felt that there has been enough change to indicate doing something now (i.e. within the next few months) rather than waiting longer within the calendar year.
Any further treatment, my doctor explained, (i.e. radiation, chemo, etc.) would depend on what they find during surgery. In other words it would depend on how much tumor they can resect as well as the status of my tumor (grade II or III) based on biopsy results. Following surgery there would be a post-op tumor board meeting and a decision would be made within a week regarding next steps for treatment. In addition, genetic testing would be used to get further details on my tumor’s molecular characteristics. While I would have next steps decided within a week after surgery based on histology (…how the tumor looks), that plan may change given the genetic markers. Regarding radiation therapy, UCSF’s radiation oncologist did not think there was a problem of doing photon reirradiation, but recommended I talk with my Boston team about proton beam therapy (…the radiation I did during my last recurrence) since they do not have proton beam in the Bay Area. Whether to do radiation a second time is a highly debated topic given the significant side effects/risks.
Before my doctor ended the call, she recommended I speak to my team of doctors in Boston to get their opinion. She mentioned there may be a scenario where the Boston team may think that a “wait and see” approach is best, which would make things particularly confusing, but I first need to wait to hear what they think. As a long-time patient, I was pretty impressed by my doctor’s honesty. Usually asking for a second opinion is a delicate and awkward exercise, particularly with specialists. Patients are often scared that getting a second opinion would look like they don’t trust their doctor and thus damage their relationship with that physician. In my experience, every now and then doctors do react poorly to requesting a second opinion, but the majority don’t mind. It is usually one of the best moves any patient can make. The more information you can get, the better.
We ended the phone call. Before I called my Mom to update her, I transcribed my notes onto my computer. For any patient reading this, I highly recommend re-writing your notes. Not only does it keep everything organized, but it importantly provides you an opportunity to digest the information, see what made sense, and ask yourself what further questions you have.
After transcribing my notes, I called my mom and primary care physician to debrief. Together, we came up with a plan to see my doctors in Boston and also made a list of questions for the neurosurgeon at UCSF. Again, for patients, similar to rewriting notes, involving others in these conversations (either as they are occurring or afterwards) helps you digest the information as well as come up with important questions you may not have thought of otherwise.
Summary:
- The growth is real and not a factor of imaging differences. It is enough growth to act now rather than wait.
- UCSF recommends surgery as the first step, but I need to meet with UCSF’s neurosurgeon
- Any further treatment would be based on biopsy results following the surgery
- I need to get a second opinion from my doctors in Boston
Meeting with UCSF Neurosurgeon (1hr 22min)
On March 19th I was scheduled to meet with the Neurosurgeon at UCSF. He is one of the leading experts on brain mapping in “eloquent areas” (i.e. areas of important function in the brain), particularly the motor cortex. Soon after my March 15th call, my Mom and her fiancé went on a trip to Costa Rica, a vacation they had been planning for a while. Given everything going on, my Mom didn’t want to go. She wanted to either stay in Boston or come to San Francisco for my meeting. I told her no. She was obviously free to do what she wanted, but I wanted her to go on vacation for me. She has been through a lot, and needed some time to decompress. Rather than have her in the States for this one meeting, I needed her to be refreshed and rejuvenated given that this journey was going to be a marathon, not a sprint. Plus, I just wanted her to go have fun! Being a caregiver is exhausting work. Caregivers often think that the people who they are caring for shouldn’t worry about their own caregiver’s wellbeing, but we do. It is better to let us as patients care for our caregivers because it is a way in which we also care for ourselves. So, my Mom left for vacation, but made sure she had a good international phone plan!
I thought I would be okay going to the surgery meeting by myself, but in the days leading up to the meeting I realized I needed someone there. In some ways I was being hypocritical. A month or so prior I went with my friend to her surgery consult after emphasizing the benefits of having a second person in the room. Now here I was thinking I could do this by myself? No way. At any consult it is important to have at least one other person there to help take notes, remind you what questions you forgot, ask questions you may not have thought of, and be there for emotional support. I realized I needed this and reached out to my Uncle in Seattle who without any hesitation made plans to come to San Francisco for my meeting.
Before we headed into the UCSF outpatient building for my appointment, I told my Uncle a set of ground rules I have for anyone joining me in my appointments. These are important to me. I vividly remember as a child my doctors ignoring me and only paying attention to my parents. Even during my first recurrence in 2014, some doctors directed their attention to my parents in the room rather than at me. From that point on I developed a system for how I like people joining me in my appointments to act. This mostly involves letting me do most of the talking without interrupting, helping redirect my doctor if their focus isn’t on me, and asking their questions only after I let them know I am done with my own questions. This may seem strict and out of character for people who know me, but it is a way I maintain my agency as a patient. It is a way I keep myself in the driver seat to my own medical care.
With my Uncle in the room and my Mom on video chat, we started the appointment discussing why the surgeon believed surgery was the appropriate first step in my treatment. He said I am at a bit of a crossroads with my treatment given current research. Previously it was agreed upon that surgery was overall beneficial for glioma-type tumors, but given the increasing knowledge of tumor diversity based on molecular mutations, there is a debate on whether surgery is as beneficial as previously thought for survival outcomes. There is very little research to support either side of this debate. The surgeon, and UCSF as an institution, believe the more you remove, the better you do. Interestingly enough, the surgeon I was planning to see at MGH in Boston is on the other side of this debate. Unfortunately, due to the sparsity of research, no one actually knows the answer. Since prior research grouped all gliomas together as the same “type” of tumor rather than parsing out the various mutation sub-types, no one knows if the extent of surgical resection affects survival outcomes. Also, most of the research related to both sides of this debate are based on newly diagnosed patients with common glioma mutations. I don’t fit into that population (an issue I will discuss further in this and additional posts.
Nevertheless, the UCSF surgeon believes surgery is the best path forward if it can be done in a way that doesn’t compromise significant function. He believes it is the best next step not only to resect as much as possible and “debulk” the tumor, but also to get a biopsy. Given that adjuvant therapies like chemo can now be targeted towards specific molecular mutations, it is important to know what type of tumor we are dealing with. The last time I had a biopsy was during my 2004 surgery, and a lot may have changed since then. Overall, what’s important to remember is that this surgeon’s goal for surgery would be both therapeutic and diagnostic.
After establishing the reasons for surgery, we discussed what it would involve. The tumor is located in the motor strip that controls mostly the right leg and part of the arm. The brain is pretty fascinating. The various locations of the motor strip can be mapped pretty consistently with what part of the body it controls. It’s called the homunculus (…see image below from Costanzo “Physiology” 5th Ed.), which literally means a “man” since it is all the parts of a person mapped out onto specific areas of the brain.
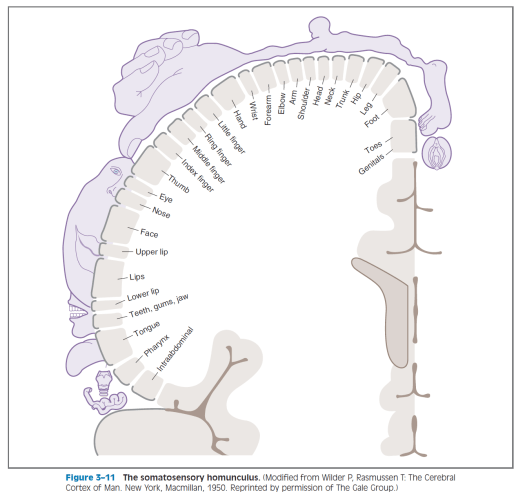
While it may seem very organized, my brain is a tad unique. When I had surgery in 2004, my brain rewired itself (…called neural plasticity) so that other parts of my brain could take over for the section that was removed. If this didn’t happen, I would have remained paralyzed on my right side. Due to this, while surgeons know anatomically that a certain part of the brain controls the foot, my brain may be different. For example, the new tumor growth is in the area that should anatomically control my leg and foot, but I am having symptoms mostly in my arm. Does this mean that area is actually controlling my arm? No one knows. These unknowns are why I need a certain type of surgery that involves intricate brain mapping.
Ready for some sci-fi, grey’s anatomy stuff? He proposed an awake craniotomy!

I would start asleep while they do what they need to do (i.e. open up my head), but then they would wake me up. While awake the surgeon, using electrodes, would send electrical signals to the parts of the brain he wants to remove to test if there is any important function there. While he stimulates these areas I would perform both active and passive tasks. Active tasks involve doing an action (i.e. opening and closing my hand) and then seeing if brain stimulation affected that action. Passive tasks involve staying still and seeing if stimulation causes involuntary movement. We would also do other tasks and stimulation related to language and cognition to test for those functions as well. If electrical stimulation to the tumor site shows no change in function, then the surgeon may resect that layer and stimulate the next layer for possible removal. This would be repeated until they reached a point that showed functional brain tissue. There would be no circumstance where my surgeon would resect a section of tissue that showed function. If everything showed function, then they would only take a biopsy to determine further treatment decisions.
You may ask, which I certainly did, “if they are using such detailed brain mapping shouldn’t there be no risk in functional loss?” Well, not exactly. While the chances of complete paralysis are low (yet always a risk), some functional deficits are possible. After surgery I will more likely than not have transient weakness that usually results from edema (…brain swelling) post-surgery, but over time that function would return as the swelling goes down. The extent of how much movement returns depends on how aggressive we are in surgery. This aggressiveness is related to the extent of tissue removal that showed no function during electrical stimulation. You see, brain mapping for function is not binary. If an area shows no function during the surgery it does not mean that the entire tissue has no involvement in movement. Removing that piece of tissue may inadvertently affect some form of movement.
To clarify, the doctor put it this way: Think of someone who is a surgeon and someone who is a baggage handler. The way they use their hand is very different, and thus may affect their level of tolerance for functional deficits. A surgeon relies on minute movements and may not be able to operate with deficits. On the other hand (…no pun intended), a baggage handler could still pick up bags even if their hand had some functional loss. The surgeon in this scenario thus has a very low tolerance of risk and the baggage handler may have a higher tolerance.
If I have no tolerance for risk then my surgeon recommended not doing any surgery since even the mapping process creates some risk. The level of risk tolerance I have will determine the surgeon’s aggressiveness of removing tissue while operating. This is a conversation he and I will have before the surgery, but also during the surgery. In fact, if there was no conversation about tolerance, this surgery would only take a few minutes to remove the tumor, but since we are discussing tolerance and mapping during the surgery, this operation takes several hours.
When I asked about recovery, he told me that he usually recommends people request three months leave from work. Fortunately, I am in one of the few medical schools (…in the world) where I have 3.5 months of summer. While we are supposed to do research for our Masters during this time, it offers an opportunity to continue with school despite the long recovery time of the operation.
I asked a lot more questions, but if I kept writing about each one, I’d likely get carpal tunnel. For informational purposes, below is a bulleted list of some questions I asked. If you would like the answers, feel free to message me:
- What do you anticipate to be the neurological deficits? If success, what are the post-op expected deficits?
- Will there be transient weakness?
- Would it require acute rehab?
- Would it need outpatient therapy?
- What about other deficits? Could there be processing/learning challenges similar to what happened back in 2004?
- Will there be transient weakness?
- How much can be removed?
- What are the risks/probabilities?
- What is the worst case scenario in terms of weakness and recovery? How long could it take to recover?
- What is the likelihood I would need to do other forms of treatment after surgery?
- Are there other options besides treatment that would provide the same or better outcome with less risks, or is surgery the best option?
- What are the consequences of not doing surgery?
- When would it be best to do surgery? Is sooner better, or could it wait until the summer?
- If I did surgery at UCSF, would he recommend recovery here? If better to recover in Boston, how long until I would be able to fly?
- In his opinion would there be a benefit to doing surgery at UCSF if I should recover in Boston, or would it make sense to do it back in Boston?
- What should I consider in making this decision?
- Are there any questions you think I should have asked? Any unknowns still that would help inform the decisions moving forward given that I haven’t yet heard from the team in Boston?
While the above questions provided A LOT of useful information, my final question was probably the most important. It is a question I ask every doctor I see when getting information for treatment decisions: “What would you do if you were in my shoes?” I ask this question not just to know what they would do, but mostly to see if they actually answer the question. Are they willing to be candid enough (…may I say human enough) to answer this question? Do they see me as a partner in my care where they are willing to be honest with me, or do they approach the doctor-patient relationship in a more protective, paternalistic manner? In the past, this question determined who I sought care from, and I wanted to see what this surgeon would say.
This was his answer: “You know, I have actually thought a lot about this question over the past few days. I figured I would continue with med school, think about what type of doctor I would want to be, and would move forward with more aggressive treatment now rather than later.”
To his last point, “now rather than later,” he was addressing a conversation we had regarding whether surgery could be pushed off. He had said it may be possible to come up with some chemo cocktail to kick the can down the road so I could finish medical school. Nevertheless, at that time not only would my schedule be more busy as a resident, but also the tumor may become too diffuse, taking surgery off the table. Waiting was not recommended.
What struck me most though in his answer was, “I would continue with med school.” I asked him, “What did you mean? How did you reason through that?” He explained that going to med school is a 10 year investment to get to a point where you can give back to your family and society. If he thought he wouldn’t have that time given his condition, he would choose to pursue something else that would let him give back to his family and society now. However, he thinks given the situation I am in, it is possible to reach that 10-year mark. In fact, going through this experience, he suggested, may make me better prepared to help my patients.
He ended our appointment mentioning that surgeons often focus on quantity of time rather than quality of life, but he thinks focusing on quality of life is just as important. In fact, he started a research program at UCSF on the cognitive aspects of brain mapping surgery since surgeons do not often take into account quality measures of risk such as cognition. As part of his program, he does a battery of neurocognitive tests and has formed a multi-specialty team that works on rebuilding cognitive function post-surgery.
Before I left he encouraged me to talk with the surgeon at MGH who actually happens to be a close friend of his back from medical training. He emphasized that decent, smart people may sometimes disagree so that I may be prepared for the scenario where the Boston surgeon’s opinion may be different from his own.
…One hour and twenty two minutes, and he only looked at his watch once. I had never in my 15 years of being a patient been offered an appointment with a doctor, let alone a surgeon, for that amount of time. It was exhausting, but immensely informative. I felt grateful for the time he spent with me.
When the surgeon left the room, I checked the recording of our conversation on my computer. It didn’t work! I slightly (…maybe more than slightly) panicked, searched every help forum for Microsoft’s OneNote, but unfortunately couldn’t find any solution. Luckily the combination of notes from my Uncle, Mom, and my own typed notes were sufficient to reconstruct the meeting. I spent some time rewriting my notes to synthesize the information. After leaving UCSF my Uncle and I went out to lunch to debrief on what we learned, and what further questions we had. We received UCSF’s opinion, and it was time to go to Boston.
Summary:
- UCSF believes the more tumor you remove, the better you do (but the details of this are currently under debate in research)
- The UCSF surgeon’s goals for surgery are both therapeutic (to offer better outcomes and/or more time between the next recurrence) and diagnostic (to get a biopsy sample to determine further adjuvant treatment)
- The surgery would be an awake craniotomy using brain mapping techniques to test for functionality before attempting to resect parts of the tumor
- While the risk of permanent functional loss is low, there is a risk of deficits
- The tolerance of risk I have for these deficits will determine how aggressive the surgeon will be
- This is a conversation that will take place before and during the surgery
- The tolerance of risk I have for these deficits will determine how aggressive the surgeon will be
- I need to get a second opinion from the surgeon at MGH in Boston
Meeting with MGH Neurosurgeon (45min)
On March 29th, I met with a neurosurgeon at MGH to get a second opinion. I was lucky to get an appointment with the same surgeon I consulted with during my recurrence in 2014. Before the appointment, MGH’s tumor board discussed my case, and I was sent an email with their recommendation:
- A surgical biopsy should be done
- Everyone recommended a course of another type of chemotherapy called PCV
- They recommended against re-irradiation
At the start of my appointment, the surgeon explained the tumor board’s recommendations. He said molecularly, I have an adult-type oligodendroglioma. The chemotherapy PCV (…which is three types of chemo: Procarbazine, Lomustine (also called CCNU), and Vincristine) should be strongly considered to close the loop on the standard-of-care approach for gliomas. Generally, the standard of care is based on evidence demonstrating the most effective outcomes. For my type of tumor, the standard of care includes surgery (…completed in 2004), chemotherapy (…temodar, completed in 2014), and radiation (…proton beam, completed in 2014). The final step is the other evidence-based chemotherapy, PCV, which I have not yet received.
After this, the surgeon addressed the elephant in the room. In 2014, him and I met for a consult and he recommended against surgery. One of my major questions, which he answered without me having to ask, was why could I have surgery now? He explained that in 2014 they were concerned that the risk of surgery was too high given the tumor’s involvement of my hand in MRI imaging. If you recall the image above, anatomically, to reach the 2014 growth that involved my hand, they would have had to go through my entire right side, likely causing full or partial loss of function in my right side. Back then, I had two options, a highly risky operation or the standard of care involving chemo and radiation. Now, the circumstances are different. I actually had a great response to the chemo and radiation from 2014, resulting in tumor shrinkage. While a full resection is still not possible, the reduction in size and change in growth direction makes surgery a possibility this time around.
He could try an operation to shave away at the tumor nodule, but there would be a risk to function. There is a chance that the neural plasticity (…previous remapping) of my brain following my 2004 surgery may be beneficial to avoid significant functional loss, but there is still a risk. Rather than trying to shave away at the tumor, he was more focused on getting a biopsy. The area of greatest concern is a linear strip that on the MRI imaging is indicative of possible tumor evolution to a higher grade. While this could be part of the natural life-course of oligodendroglioma tumors, the temodar treatments may have caused part of my tumor to hypermutate. While most of the tumor looks historically similar to what I’ve been dealing with since 2004, it would be important to know if there has been any hypermutation because it would change how we approached treatment. The only way to know if this area is hypermutated would be to do a biopsy.
I was a little confused what his goals were for the surgery. Did he want to try to resect as much tumor as possible while getting a biopsy, or just focus on getting a biopsy? He clarified that it would not be a good idea to go into surgery with the idea of a maximal resection. Instead, it would be better to do a biopsy procedure. The advantage of this is to understand the pathology of tumor to choose targeted therapies. Overall, his goal would be diagnostic, but would try to remove tumor that wouldn’t compromise permanent functional loss. Even with an attempt at a large resection, I would need further treatment since it is impossible to remove all the tumor given its location and tentacle-like nature. When I compared his goals to the surgeon at UCSF he emphasized his goals are not therapeutic. His focus is a diagnostic surgery followed by PCV, knowing that therapeutic-type surgery would be needed down the road. Give my high functionality, he would wait to do surgery that would risk any deficits now so that I could utilize my current function. He is unsure how much surgery really provides benefit to overall outcomes (…the research debate I discussed previously).
We moved the conversation forward to what the surgery would involve. He said it would be relatively safe without much risk of permanent deficits. The type of surgery would be pretty much identical to the procedure UCSF suggested. The only difference, he said, was that he does his brain mapping solely with electrodes while keeping the patient asleep the entire operation. To me this seemed like a big difference to UCSF, but he calmly said that the decision to do an awake vs. asleep surgery is simply a matter of preference. There’s no difference in outcomes or risks. Since I would be asleep throughout the surgery, I wondered how language and cognition could be tested. He responded that he viewed this surgery as solely motor and that language testing during motor mapping was an institutional difference between MGH and UCSF (…I later asked the UCSF neurosurgeon about this and he agreed that the surgery was mostly motor and the difference in method was not significant).
Like all motor surgeries the worst case scenario was paralysis, but this is highly unlikely. Instead, he said the risk of transient weakness of my arm and leg is pretty fair. This is due to what is called a post-surgical Todd’s event. When I have focal seizures in my arm, I temporarily loose movement, and as function comes back it remains weak but eventually returns to normal. This is called Todd’s paralysis. To simplify, it occurs because the neurons controlling movement get tired after all of the hyperexcitation from the seizures. During brain mapping they send a lot of electrical shocks to my neurons, which similarly exhausts the neurons and results in transient weakness post-surgery. As the surgeon described, it’s like my brain goes through about 1000 pushups. This weakness generally subsides within a few days, and therapy helps maintain function.
After talking logistics, I shifted our conversation back to his views on the benefits of surgery. He said that surgery is known to be beneficial for astrocytic (…higher grade) tumors, but it us up for debate whether its beneficial for lower-grade tumors. Usually oligodendrogliomas with my molecular make-up manifest in people who are already in their 60s. In this case surgery is usually not done. Why take the risk when an older person is more likely to age and face debilitation or mortality due to normal aging processes rather than the tumor itself? My case is difficult though since I developed an adult oligodendroglioma as a kid. Given the greater length of time it is in my head, the probability of it evolving is higher. Do I then match more with the astrocytic tumor groups or with the older low-grade oligo populations. There’s no answer because in general there is very little research. Even within the existing research, I don’t fit into any of the populations assessed.
The surgeon was confident in the benefits of PCV, so I asked if it would be better to do PCV first to shrink the tumor rather than starting with surgery. He said there’s no answer. No matter what, there will always be tumor cells left. It will continue to come back. This is partly why the MGH tumor board recommended against radiation. They want to keep that option for later down the road when I run out of other treatment options. Essentially this is like a game of chess. I have to figure out when and how to play my pieces, and in my case, these pieces are the various treatment options I have at my disposal. In the future, when the tumor grows again I should expect functional deficits at some point simply because it would start interfering with the neurons in my brain. So how do I play my chess pieces now? In this surgeon’s opinion he wonders why take the risk of an aggressive surgery when we know I responded to chemo in the past. The only reason surgery is an option now is because I responded to chemotherapy. This is why he wants to focus on a biopsy and then PCV chemotherapy.
When I asked, “what would you do if you were in my shoes?” He answered, “do what you are doing now, and keep talking to all the doctors.” When I pushed him a bit more, he clarified he would either do PCV with no surgery or a diagnostic surgery followed by PCV. He would give PCV a chance before aggressive surgery. If the PCV ends up not working or whenever the tumor recurs, then that is when he would consider more aggressive surgery that would likely result in functional loss.
After forty five minutes of conversation the surgeon had to leave. I was immensely grateful for the amount of time he gave me to ask my questions, but I was also a bit bewildered. To me, it seemed like this surgeon at MGH and the surgeon at UCSF had two vastly different opinions. They both recommended surgery to get a biopsy, but the surgeon at UCSF also had a therapeutic resection goal, whereas MGH did not. These differences in goals were a result of the larger debate on the benefits of surgery for low-grade gliomas. On one side is UCSF that believes the more you remove the better you do, and on the other side is the surgeon at MGH who questions the efficacy of surgery towards survival outcomes. No one knows the answer. As the surgeon at UCSF said, “decent, smart people may sometimes disagree.” He was right. So how do you make a decision when there is no right, or wrong, choice? I needed to go see Yoda (i.e. my neurooncologist at Dana Farber).
Summary:
- MGH believes a biopsy is important, PCV chemotherapy should be used, and I should not get radiation right now.
- MGH’s surgeon isn’t sure if a resection-type surgery is beneficial to survival outcomes. Surgery is possible now since I responded to a combination of chemotherapy and radiation in 2014. Why risk function I have now, when I still have the option of PCV. His goal for surgery would be solely diagnostic in order to get a biopsy to direct further treatment.
- I would be asleep during the surgery, but it would essentially be the same brain mapping surgery proposed by UCSF. The difference between being awake and asleep during the surgery is entirely stylistic and does not differ in regards to risk and/or outcomes.
- The risk of permanent functional loss is low, but there would be some transient weakness that I would likely quickly recover from.
- Essentially, let PCV have a shot at the tumor before relying on a more aggressive approach to surgery.
- The goals of the UCSF and MGH surgeons slightly differ since the research, and where I fall into that research, regarding the benefits of surgery to overall outcomes is unknown.
- I need to go see Yoda (i.e. my neurooncologist at Dana Farber).
Meeting with Dr. Wen (a.k.a. Yoda) at Dana Farber (47min):
Right after finishing my appointment at MGH, my family, primary care physician, and I headed straight to Dana Farber for my neuro-oncology appointment.
There is something uniquely calming about seeing Dr. Wen. You may notice he is the only doctor I name in this post. This is simply because I have not had a chance to ask the other doctors their permission to include their names. Dr. Wen on the other hand has been featured in my blog before. I don’t call him Yoda for just any reason. He is one of the most wise, sincere, and empathetic doctors I know. Also, like Yoda, his voice and presence is incredibly soothing (…in grammatically correct sentences…unlike Yoda). Finally, he is probably the best at replying to emails compared to any other person I know while at the same time directing Dana Farber’s Neuro-oncology Department, and serving as one of the world’s leaders in brain tumor research. There is no other way he can do everything without using The Force.
Now back to what happened: Our appointment began with discussing whether or not surgery should be the first step. In his opinion, the benefits of getting a biopsy outweighed the risks in order to get a sense of what we are dealing with. The next decision to be made beyond a biopsy is how aggressive I should be in surgery. He believes that if it is safe to resect more than just the tissue needed for the biopsy then that would be to my advantage. He emphasized he wouldn’t risk permanent functional loss for greater resection, but removal beyond a biopsy may offer some modest benefits. When I told him MGH’s opinion about waiting to do more aggressive surgery until after seeing the effectiveness of PCV, Dr. Wen responded that this may likely be my last surgery. I paused, surprised by his response, and asked what he meant. He explained that if my tumor continued to grow it may grow further into the motor strip and thus impossible to remove. While I could choose to give up movement in my arm or leg to remove the tumor, he emphasized that my quality of life in the future was just as important as it is now. He doesn’t think it would be worth purposefully sacrificing movement now or later. His response made sense, but the idea that this may potentially be my final shot at surgery was unsettling.
Given that all three institutions (…UCSF, MGH, and Dana Farber) recommended at least a biopsy, Dr. Wen and I shifted our discussion towards how the tissue sample will inform treatment options. Most importantly, we need to know whether the tumor has hypermutated, which can occur naturally or at times following temodar chemotherapy. Additionally, an important factor for treatment is whether the MGMT promoter sequence is methylated or unmethylated. Before I jump into those details, let me take a step back. In 2014, Dana Farber as part of a research study, sequenced my tumor from 2004 that was stored somewhere in the basements of MGH. The molecular study report revealed the following:
Molecular study report from 2004 tissue sample:
- 1p/19q whole arm chromosomal co-deletion (characteristic of adult tumor)
- Combined loss of 1p and 19q is commonly found in adult patients with oligodendrogliomas, and is a common molecular signature for oligo tumors.
- Kids that have oligo tumors usually do not have this co-deletion.
- MGMT promoter-unmethylated
- MGMT (O6-methylguanine-methyltransferase) promoter methylation occurs in the majority of adult oligo tumors, and is often positively correlated with 1p/19q loss.
- IDH1 mutation – negative (characteristic of pediatric tumor)
- IDH1 (isocitrate dehydrogenase 1) mutation has been found in many adult oligo tumors, and commonly associated with the 1p/19q deletion.
- Adults tend to have this mutation.
In addition to the above results, they found that while I do not have the IDH1 mutation, I do have the IDH2 mutation. Usually most people have either both mutations or none, so to have only the IDH2 mutation is pretty rare. Given the paucity of research and the molecularly “unique” nature of my tumor, it is difficult to make treatment decisions. While my tumor is characteristic of an adult-type oligo, I was originally diagnosed as a child. In addition, I have the rare IDH mutation combination. Combine all of this together, and I do not fit into any previously or currently studied research population.
Dr. Wen was most concerned about the unmethylated MGMT promoter. The research on the relationship between these molecular features and treatment effectiveness is relatively new. Recent research has shown that chemotherapy is more effective for glioma tumors with methylated MGMT promoters. My tumor is unmethylated. During my last round of genetic sequencing, only two of the four samples were high enough quality to produce results, so it is important to get a new biopsy to clarify my tumor’s genetic make-up. If it is true that my tumor is MGMT-unmethylated then Dr. Wen is less optimistic about the benefits of PCV chemotherapy.
Even though he would be less optimistic about PCV, we would still try that approach in order to close the loop on the standard of care. The research on treatment effectiveness is population-based, so I can potentially fall to either side (…better or worse) of the average response. If we were to do PCV, Dr. Wen suggested only using the first two chemotherapies in the acronym: “P” and “C”. “V,” or Vincristine, doesn’t cross the blood-brain barrier, and has the greatest side-effects. Even though the clinical evidence of PCV effectiveness for gliomas involved Vincristine, Dr. Wen is skeptical of its use. Outside chemotherapy, he agreed with MGH’s recommendation that we should save radiation for a later recurrence when there are less options available. In fact, he believed the proton beam therapy I received in 2014 is most likely the reason for my tumor shrinking, rather than the temodar, but there is no way of knowing which one had a greater impact.
If the biopsy shows that the tumor has evolved in grade or hypermutated then Dr. Wen would not recommend chemotherapy as the first step. Instead he would do immunotherapy since the research shows that hypermutated tumors are immunogenic (…able to produce an immune response) and thus may be responsive to immunotherapy. While immunotherapy is not clinically used for brain tumors, both Dana Farber and UCSF have trials using immunotherapy for hypermutated glioma tumors. If needed, I may qualify for these trials.
Beyond the immunotherapy trials, Dr. Wen discussed additional clinical trials. Most of these are IDH inhibitors that target the IDH mutations I discussed previously. Unfortunately, most of these trials focus on IDH1 mutations and not IDH2. Given that I only have the IDH2 mutation, I do not qualify for these trials. Despite this, the treatments in these trials do include FDA-approved IDH2 inhibitor medications. If the standard of care doesn’t work for me, I could try to get the IDH2 inhibitor treatments off-label (…beyond what they were originally approved for). This would require asking AGIOS (…the pharmaceutical company making these drugs) to release the treatment on a compassionate care basis since insurance does not cover off-label use. Another trial coming down the pipeline is related to PARP inhibitors. A Yale paper released in 2017 found that PARP inhibitors (…traditionally used for people with the BRCA gene in breast cancer) may work for IDH mutated brain tumors. While the clinical trial has not yet begun, the lab data has been particularly encouraging. The pace of research and clinical trial progress is incredibly encouraging; however, as Dr. Wen explained, all of this is uncharted territory. These trials would be the next step after whatever “standard” approach (chemotherapy or immunotherapy) we choose for my current recurrence.
Regardless of whether I need chemotherapy or immunotherapy, I would begin one to one and a half months after surgery. I asked if I could stay in school during these treatments and Dr. Wen said it is possible, but would depend on how my body reacts.
Like all of my past appointments, I asked Dr. Wen the golden question: “What would you do if you were in my shoes?” He said he would do the surgery to get a biopsy as well as see how much tumor they could remove without purposely risking permanent functional loss. Additionally, he would continue with chemotherapy or immunotherapy depending on the biopsy results while also asking AGIOS for compassionate care release to prepare for future scenarios where I need access to these clinical trials.
The talk of all these treatments and clinical trials brought to mind the UCSF surgeon’s comment regarding the 10-year investment towards staying in medical school. I wanted to know if Dr. Wen agreed whether or not I have that time to invest. He said it’ll be important to see what the biopsy results show, but for now I should keep doing what I’ve been doing. Even though he thinks I should have stayed in Boston for medical school (…a running joke of his), he encouraged me to go back to San Francisco and the life I have developed there. Regardless of where I choose to do my surgery and treatments, he emphasized he would continue to be part of my team.
Summary:
- Recommends at least a biopsy, but it may be beneficial to remove more tumor without purposely risking permanent functional loss
- Given that my tumor was and may still be MGMT-unmethylated, he is less optimistic about the effectiveness of chemotherapy like PCV
- If the tumor has hypermutated/evolved in grade, I should do immunotherapy rather than chemotherapy. If it has remained the same then I should do the “P” and “C” part of PCV
- Regardless, I should start thinking about clinical trials for the future. While I may not qualify for some of the trials given that I have a rare IDH mutation combination (IDH2 but no IDH1 mutation), I should contact AGIOS to request compassionate care release for future use. This would only be considered after completing the standard of care
Debrief with my family and PCP:
After finishing a whirlwind of appointments at MGH and Dana Farber, my family, primary care physician, and I went to Dana Farber’s cafeteria to debrief on everything we learned. We agreed that all three institutions (UCSF, MGH, and Dana Farber) recommended obtaining a biopsy of the tumor. UCSF’s goal of the surgery would be both therapeutic and diagnostic while MGH’s goal would be solely diagnostic. UCSF definitely has a more aggressive approach while MGH is more conservative and focused on PCV chemotherapy. Interestingly, Dr. Wen is less optimistic about the effectiveness of PCV given that my tumor is likely MGMT-unmethylated. While UCSF and MGH’s surgical recommendations may seem significantly different, neither of the surgeons would want to do a resection that purposely causes permanent functional loss. This is also Dr. Wen’s view of surgery. Biopsy is the goal, but further resection would be good if the risk isn’t too significant. While I had collected a ton of information and wanted to ask more questions, there was really only one question that mattered at this moment. Since I needed to have surgery for a biopsy regardless of whether or not I attempt further resection, I needed to choose who I wanted to do the surgery.
My primary care physician, who has been amazing throughout this entire process, presented me the following hypothetical: “If both surgeons were in Boston, who would I choose?” Immediately as he said this, I knew my gut pointed to UCSF. This was a personal decision and not based on the quality or ability of either surgeon. In fact, both surgeons said they would have the other surgeon operate on their family. If you would like more information on why my gut went for UCSF, please send me a message and I’d be happy to share. What’s more important to explain is why was this question THE question given everything I had learned over the past couple weeks. My doctor explained, given that surgery was a definite, I needed to go with whichever surgeon felt better in my gut. Since every surgery involves risks, if in the small chance something was to go wrong, I wouldn’t want to question my decision afterwards.
It was a bit surreal that after all the information and copious notes I collected, the next step simply came down to that single question. While I knew that my gut was pointing to the UCSF surgeon, I had a few more questions for UCSF and Dr. Wen before finalizing anything.
Clarification calls with UCSF Surgeon and Dr. Wen:
I was a little concerned with how polar UCSF and MGH’s surgical goals were. While I knew neither wanted to cause permanent functional loss, UCSF was definitely a more aggressive mindset. I talked with the UCSF surgeon on the phone to clarify his intentions for the surgery. He reinforced that his goals were not just diagnostic, but also therapeutic. Even though this was different than MGH, he would never purposely cause functional deficits to remove more tumor. There is a spectrum of risk between just doing a biopsy and trying to remove a lot of tumor. The degree of risk within this spectrum depends on my level of tolerance. I can decide I don’t want to take too much risk and just do a biopsy, or I could say I’m willing to risk some deficits to attempt a greater resection. That would be up to me and a conversation I would have before and during the surgery.
I also had a call with Dr. Wen at Dana Farber to clarify his views on surgery. He said the data on surgery effectiveness for recurrent gliomas is not great. For new diagnoses, biopsies are less effective than partial resections, which are less effective than total resections. That, however, doesn’t necessarily apply to recurrences since research on this has only focused on newly diagnosed patients. I also wanted to ask Dr. Wen if he thought UCSF and MGH’s surgical recommendations were as different as I thought. He didn’t think they were too different since both would want to resect tissue if possible without compromising permanent function. The difference is slightly nuanced and in some ways I was splitting hairs. Additionally, he reinforced that if the tumor is still a low-grade MGMT-unmethylated oligodendroglioma, he is less optimistic about the effectiveness of PCV chemotherapy, so if possible, the more tumor that can be removed the better. A temporary decrease in strength/function that would eventually come back is an acceptable risk for surgery, but I should not consider long-term functional loss for greater resection. During our meeting in Boston I noticed his demeanor seemed less optimistic (which may have been the jet lag after returning from China the day before). I wanted to get a better sense though of how he felt about my situation. He clarified that he is actually hopeful given all the new trials coming down the pipeline that I may need at the time of my next recurrence (…something I will discuss more in future posts).
After finishing both calls I finally had answers to all my questions. My gut feeling had not changed, and I was going to get surgery at UCSF.
Summary of Treatment Plan:
I didn’t realize how long this post would become, and how many details there were in all my appointments. In total I had about 4 hours of calls and in-person meetings. I posted all the above information to help anyone who wants to know what type of questions and conversations go into making treatment decisions. First, I’d like to emphasize my positionality in all of this. Few people get the amount of time and access to seek opinions from some of the world’s top doctors and institutions. My opportunity to collect 4 hours of information is an immense privilege rooted in many facets of my identity (…something I’ll discuss in later posts).
If you made it this far, or are simply skipping down to this section, below is a summary of my treatment plan:
- I will undergo an awake brain mapping surgery at UCSF on May 22nd to get a biopsy and attempt a partial tumor resection
- Before and during the surgery I will have a discussion with my surgeon about the level of risk tolerance I have in order to determine how much tumor we resect beyond the biopsy
- I will be in the hospital anywhere from 2 to 7 days
- Depending on how the surgery goes, I may need inpatient rehab, but the surgeon thinks this is less likely
- The overall recovery period will be about 3 months, but there will be an intensive outpatient period for 2 to 4 weeks where I will need help with daily living tasks and rehab for any transient weakness after the surgery.
- Within a week or two I should get pathology results of the tumor to learn whether the tumor is still a grade II oligodendroglioma or if parts of it have evolved. About three weeks after surgery, I will get the molecular results of the genetic sequencing.
- If the tumor is still a grade II oligodendroglioma then I will do PCV chemotherapy (or just the “P” and “C” part)
- If the tumor has evolved and hypermutated then I will do immunotherapy
- The above adjunct therapy would start about one to one and a half months after surgery
Essentially after over 9,000 words summarizing copious notes, the only known factor of all this is that I will have surgery at UCSF on May 22nd. Anything that happens after that is unknown until we see how I come out of surgery and what they find during the biopsy.
While I have the option to do recovery and rehab in Boston after the surgery, I decided to stay in San Francisco. This was not an easy decision, and required a lot of thought and reflection. To give it justice, I will save why I decided to stay in SF for my next post.
Final Tips for Patients:
- During these appointments I had the advantage of having gone through all of this before, so I was able to pull upon past lessons on how to approach these meetings. Below are some suggestions I have for anyone going through similar experiences:
- Make a list of questions before your appointment. Review these questions with people you trust (family, friends, your primary care physician) and ask what other questions you should add.
- Take your own notes during the appointment
- If you take notes on paper, rewrite them on the computer to help digest the information, see what makes sense, and figure out what further questions you have
- If you take notes on the computer take some time to rewrite the notes in longform for the same reasons in my point above
- Have at least one other person join you in the appointment to help take notes, remind you what questions you forgot, and serve as emotional support
- BUT don’t be afraid to set your own ground rules for how you want the appointment to go
- Collect their notes after the appointment and compare them to your own. What’s similar, what’s different?
- Ask the physician if you can record your appointment since it is a great tool to refer back to if you forgot something
- CHECK that the recording is working before realizing after an hour and twenty two minutes it didn’t 😦
- Debrief your appointment with someone else after it ends to discuss what happened. Sometimes people hear things differently in the emotionally-charged settings of these appointments, so it is good to get on the same page
- Don’t be afraid to ask for a second opinion. In fact, if you are able, I’d recommend always doing this
- If you have any further questions, email or call your physician to make a time to talk with them again
- Get sleep and watch a movie/favorite show when you’re stressed
- Most of all, trust your gut!

Dear Jeremy,
Thank you for sharing your life journey.
My heart goes out to you.
My prayers for your recovery and strength to go through the treatment.
Focus on the present and what is possible.
TAKE CARE.
Prof.R.Srinivasa Murthy, Bangalore, India.
LikeLike
Dear Jeremy,
We are all thinking of you, and hoping that the surgery is as successful as it possibly can be. Thsnk you for sharing your journey with us.
Stephanie (David’s cousin)
LikeLike