
Note: I would like to mention that all my medical results, doctor’s recommendations, and treatment decisions are my own personal experience. Each individual’s medical journey is unique. What I write is not an endorsement or recommendation for what anyone else should do. Rather, this blog serves as a window for my community, you, or someone you may know to get a glimpse into my experience living with brain cancer. Hopefully there are parts of my story that resonate, areas of connection particularly in the emotional aspects of cancer, that may be helpful to you. If you ever have questions related to what I write, please contact me.
I don’t intend to turn every post into a fundraiser, but hopefully the information I share below epitomizes why funding for brain tumor research is so critical. Sunday, June 24th is the National Brain Tumor Society’s Bay Area Brain Tumor Walk where I will be the guest speaker. Please consider donating to, or better yet fundraising for, Team Jeremy so that these seas of treatment can become a bit more charted.
Recap:
In my last post, Sailing New Seas: My Biopsy Results and The Need For a Cure, I recounted my experience receiving news that my tumor has evolved to a grade III anaplastic oligodendroglioma. Given this news, the path of treatment is uncertain. UCSF’s tumor board had one recommendation while my doctors in Boston had an alternative view. Each opinion is equally reasonable. The difference lies in the fact that I am now in uncharted waters. There’s no map navigating me to my destination. In fact, no one truly knows where we’re heading. All I know after receiving my results was I needed to find a captain for my ship, so I met with Yoda.
If you made it through my monster post before my surgery, Treatment Meetings and Plan, you know that Yoda’s real name is Dr. Patrick Wen, my NeuroOncologist at Dana Farber. As a quick recap from that post, “(…with his permission) I don’t call him Yoda for just any reason. He is one of the wisest, most sincere, and empathetic doctors I know. Also, like Yoda, his voice and presence is incredibly soothing (…in grammatically correct sentences…unlike Yoda). Finally, he is probably the best at replying to emails compared to any other person I know while at the same time directing Dana Farber’s Neuro-oncology Department, and serving as one of the world’s leaders in brain tumor research. There is no other way he can do everything without using The Force.”
In order to focus on my conversation with Dr. Wen I decided to record our hour-long appointment rather than risk getting distracted taking notes. I’ve just finished going back through the recording, taking notes, and would like to share what was discussed.
Choosing my Captain…Clarifying my Values:
Since starting my journey when I was 12-years-old, one of the most important factors in choosing which doctor I wanted to be with was whether or not they treated me as a partner in my care rather than just a patient. Since first meeting Dr. Wen in 2014, he has treated me like a partner through building trust, and most importantly, listening to and acting upon my core values I share with him.
When I received my biopsy results last week, I spent quite a bit of time thinking about my values. What is most important to me as I begin this new path, not just for treatment, but for my life? I first started thinking about this during my recurrence in 2014, and over time the tangible uncertainty of my life has afforded me the opportunity to reflect, build upon, and refine these values. To ensure my relationship and treatment decisions with Dr. Wen are going to be a true partnership, I wanted to share with him my two most important values:
- Nurture my quality of life: Given that I don’t know how long I have or whether any of the treatments will work, what is most important to me is prioritizing my quality of life. To continue living in the present, to create the space to foster and embrace my relationships, and if I have the time, to fulfill my dream of having my own family. Beyond any academic and career pursuits, this is what I value most.
- Use my experience to help others: Few have gone through living with brain cancer since being 12-years-old. To be honest, I can’t really remember what life was like before cancer. More so, even fewer people have benefited from the level of access I’ve had to the world’s best medical professionals, technology, and resources. To choose my care based on my gut feeling is a privilege I will never take for granted. Whenever the time comes that I reach the end of my journey (…soon or a long way down the road), I need to know that I used, to the best of my ability, the knowledge, experiences, and privileges I’ve gained to improve the lives of others.
What is my New Normal?
Quick Note: Parts of this blog may get a bit jargony medical-wise (…a symptom of being a medical student). If you have any questions, don’t hesitate to leave a comment at the end of the post or contact me.
After clarifying my intentions for our partnership, I asked Dr. Wen to explain what my biopsy results mean. What is this new normal I need to navigate, and what are the tools we have at our disposal?
As my doctor at UCSF also explained, Dr. Wen said that oligodendroglioma tumors over time become more aggressive and accumulate other molecular alterations that cause it to change grades. My tumor was originally a low-grade oligodendroglioma, and at some point it evolved to a higher grade. He pointed out that even though my tumor has evolved, the changes are not as drastic as they can sometimes be.
NeuroOncologists and Pathologists use what is called an MIB-1/Ki-67 index, which essentially is a measure of the proliferative activity (growth-rate) of tumors. Low-grade tumors often have an MIB of less than 5%. My pathology report came back with a range of 10-15%. Anaplastic oligodendrogliomas (based on some of the literature I perused) can average around the 20s and progress even higher. While most doctors wouldn’t call an evolved oligodendroglioma a glioblastoma (…the most aggressive type of brain tumor), oligos can eventually function similarly and reach a growth rate comparable to a glioblastoma.
My tumor, while now a higher-grade, is still a relatively slow-growing tumor compared to other types of gliomas and tend to respond to treatment. There are a few caveats to this that I’ll explain below. Overall, the goal of treatment is to slow down or arrest the growth of my tumor before it keeps evolving into a more aggressive form.
Treatment Plans:
- Plan A: IDH2 Inhibitor
- Plan A-: Immunotherapy
- Plan B: Reirradiation and CCNU chemotherapy
Plan B Reirradiation and CCNU Chemotherapy:
I’m going to start with Plan B because understanding this will help explain why Dr. Wen is proposing either Plan A or Plan A-. To begin, UCSF’s tumor board proposed plan B as their treatment recommendation because it is considered the conventional approach (with the most evidence) for post-surgical treatment. Dr. Wen explained that this plan is completely reasonable, and if I went around the country, most people would recommend this route of treatment.
There are a couple of reasons though leading to why I am not going straight with plan B: I’ve already had radiation, and it is unclear if my tumor will respond to CCNU chemotherapy. The evidence for plan B is based on newly diagnosed brain tumor patients who have not had prior radiation, and generally have favorable molecular characteristics. I don’t fit into any of those boxes. This is my second recurrence, I’ve had radiation before, and from sequencing my tumor in 2014, we know my tumor has a rare combination of molecular components.
Reirradiation comes with some risks of causing brain tissue damage. While these risks are small for a second round of radiation, given the location of my tumor in the motor cortex, they are important to consider.
The most significant factor in considering this plan is my potential lack of response (chemo-sensitivity) to the CCNU chemotherapy due to a molecular component of my tumor genome, O (6)-methylguanine DNA methyltransferase (… or more simply MGMT). The MGMT gene codes for a protein that can help repair a cell’s DNA. This gene can be methylated or unmethylated. If it is methylated the gene is silenced (…like an off button), and cannot produce the protein to repair DNA. If it is unmethylated (…like an on button), it can produce the protein to repair DNA. Usually, in my type of tumor, the MGMT gene is methylated. This is good for the tumor’s response to chemotherapy because chemotherapy damages DNA to kill tumor cells. If the MGMT gene of those cells are methylated then it cannot repair the DNA and thus the cell dies.
My tumor is unfortunately MGMT-unmethylated. While prior research involving CCNU chemotherapy didn’t really look at MGMT factors, recent research on glioblastomas (including a 2017 New England Journal of Medicine article on recurrent glioblastomas) were clear that MGMT-unmethylation has a poor prognostic factor for chemotherapy response. Research; however, is always based on statistics, so just because I have a less favorable genetic make-up doesn’t mean I definitely would not respond well to chemotherapy. I could fall above the average and respond great! The research just suggests that my chances of responding great to the chemotherapy are less.
Reirradiation and CCNU chemotherapy is something I can do if that’s the only options I have (…and may likely be something I try down the line), but if I have other choices (Plan A or Plan A-), it may be worth considering those routes first.
Plan A IDH2 Inhibitor:
Before jumping into the details of this treatment, it would be beneficial to explain what IDH is and how IDH mutations relate to brain tumors. For the purpose of this post, IDH (or Isocitrate dehydrogenase) is a protein involved in a variety of important biological pathways in the human body. There are IDH1, IDH2, and IDH3 molecules. When looking at brain tumors, we’ll focus on IDH1 and IDH2. A cell with a mutation in IDH1 and/or IDH2 can lead to uncontrolled cell division, and thus cancer.
Here is a simplified figure showing the pathway of how an oligodendroglial cell (a type of brain cell) with an IDH mutation can lead to an oligodendroglioma:
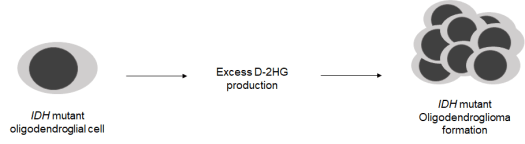
As you can see from this figure, if an oligodendroglial cell has a mutation in IDH, it ends up producing too much D-2HG (2-hydroxyglutarate). It is the excess production of D-2HG, and subsequent steps involved in cell-division control that leads to the formation of an oligodendroglioma brain tumor. An important thing to note is that IDH mutations causing cancer are not limited to brain tumors, but are also drivers of other types of cancers in the body.
The discovery and understanding of IDH mutations causing brain tumors is relatively new. This is a testament not only to the speed in which brain tumor research is developing, but also the potential for new discoveries and better treatments if we continue to invest in research.
So, now that we have the quick biology lesson out of the way, what does this mean for me? Well, most people with glioma brain tumors have an IDH1 mutation and/or a mutation in both IDH1 and IDH2. Since my tumor really wants to be unique, I have a rare mutation pattern where I only have an IDH2 mutation. This is an issue because the eligibility for clinical trials to target IDH mutations are focused on people with the more common mutations (…those with IDH1 and/or both IDH1 and IDH2).
During my recurrence in 2014, Dana Farber was part of some of the first trials involving drugs called IDH inhibitors for brain tumors (see figure below):
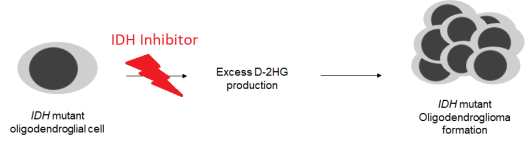
The IDH inhibitor is the lightning bolt, and in tumors that have the IDH mutation, the drug is meant to block the pathway that leads to tumor growth. These treatments don’t shrink tumors; rather, they are meant to stop tumor cell growth.
Dr. Wen and Dana Farber have a lot of experience with IDH1 inhibitors. Since starting their initial trials for people with the IDH1 mutation, they found for tumors that were not too aggressive, and did not have a lot of other molecular mutations causing tumor growth, at least half or more than half of patients had a growing tumor that just stopped growing. In fact, there are some people who have been on the IDH1 drug for 2-3 years with stable disease (i.e. no tumor progression).
No one, including Dr. Wen, has a lot of experience with IDH2 inhibitors because it is such a rare mutation pattern. The drug was initially developed for and proved to be effective for Leukemia patients where IDH2 mutations are much more common. In fact, it was actually the first IDH inhibitor to be FDA approved. Dr. Wen has used the IDH2 inhibitor in trials before, but only for a couple glioblastoma patients as a last ditch effort for those with no other options left. I am in a much different point of my illness than those patients, and the hope is given that the IDH1 and IDH2 pathways are roughly the same, perhaps the IDH2 inhibitor could put off needing other treatments for quite a while.
I won’t lie though, this is completely uncharted waters, but Dr. Wen’s recommendation for this approach is one based on the most up-to-date science available. As I mentioned in my last post, this is part of Dr. Wen’s artistry in medicine.
Given that I am not eligible for existing clinical trials using this drug, I need to try to get the IDH2 inhibitor off-label. Off-label means using the drug for purposes beyond what the FDA originally approved it for. Sometimes, insurance may just cover the drug, but usually getting a drug off-label requires the doctor to write a protocol for what is called compassionate care use. This involves getting the protocol approved by the medical institution the doctor resides, sending the protocol to the FDA for approval, asking the pharmaceutical company who owns the rights to the drug to release the drug, and seeing if insurance will cover the drug at an affordable price. The FDA actually approves approximately 99% of compassionate care requests. Thus, the biggest hurdle in this process is the pharmaceutical and insurance companies.
Plan A, this IDH2 inhibitor, is all predicated on being able to get access to it. If I can get this drug, what does it involve? Surprisingly, it is relatively simple. It isn’t like chemotherapy where you take it in cycles. Instead, it is a medication you take daily similar to how I take my seizure medications every day. Fortunately, it is also pretty well tolerated with few side-effects. While I would need to get monitored frequently, it would be possible for me to do this treatment in San Francisco with Dr. Wen in conjunction with my UCSF doctor. I would then take this drug for as long as it helps me and does not cause any significant side effects.
Plan A- Immunotherapy:
When I had my surgery last month at UCSF, samples of my tumor were taken for genetic testing. UCSF has one of the most comprehensive genetic sequencing panels to look at around 500 different potential mutations that may exist in the tumor.
These genetic results, which I hope to have within the next week, will be critical to determining whether we go with Plan A or Plan A- since it will inform to what degree the tumor is mutated. If there are not multiple mutations, then Plan A is my best bet. However, if the tumor is hypermutated, then Plan A-, immunotherapy, is the best course of treatment.
Why is there a minus with immunotherapy? Essentially, we don’t want the tumor to have a lot of mutations. The more mutations there are, the more pathways exist for cells to divide uncontrollably, causing the tumor to keep growing. The IDH mutation pathway I described above is just one pathway that can cause tumor growth. If there are other mutations, other pathways open, then even if we block the IDH pathway, the tumor still has other avenues to keep growing.
While we don’t want the tumor to be hypermutated, there are already approved immunotherapy treatments I would have access to if this is the case. Immunotherapy utilizes your body’s natural immune system response to target cancer cells. I won’t go into the details of this treatment in this post, but I’ll give a quick analogy explaining the difference between the targeted therapies and immunotherapy (…credit for part of this has to go to my friend Claire):
Imagine you have a lawn (…your brain) with a lot of weeds (…cancer cells). If all those weeds were the same type of weed, perhaps dandelions, then you can get an herbicide that targets those weeds to clean up your lawn (i.e. the IDH2 inhibitor). On the other hand, if your lawn has a lot of different types of weeds (…your lawn is hypermutated) then a single type of herbicide (…or targeted therapy) may not suffice (…I don’t know how selective herbicides actually are, but go with me on this). That’s when you need to get a goat…yes, a goat! Goats are part of the natural ecosystem (…like immune cells of your body) that already know from evolution what to eat and what not to eat. They’ll go into your yard and gobble up all the different weeds there are (…I also don’t really know how picky goats are, but for this analogy let’s assume they’re not picky). As a tangent, you can actually rent goats in Berkeley for this very purpose (…to eat grass, not cancer cells)!
Similar to the IDH2 Inhibitor, immunotherapy is generally well tolerated, but there are a few more side effects in cases where your immune system becomes overactive and attacks different parts of the body (…the goats get out of control)! Thus, I would need to get checked periodically if this is the treatment route I need to go with, but I could also possibly do this back in San Francisco too.
Why these options in this order?
My primary care doctor summarized this best. Conventional radiation and chemotherapy will shrink the tumor, whereas the more experimental treatments like the IDH inhibitor will stop the tumor from growing. If I try the chemo/radiation first, and it is not as effective as we want it to be, then the tumor may grow and mutate. If this happens, then I won’t get as much benefit from more targeted therapies. At that point, I may be trying to stabilize something that is bigger and more problematic.
The point I am at now is likely the most minimal disease I will have, so it makes sense to try approaches that arrest cell growth while knowing that I always have the opportunity to do radiation and chemotherapy.
If we looked at standard treatments, I don’t have many left. There is the reirradiation, CCNU, and also a drug called avastin that I don’t need to go into now. From this perspective, there are a limited amount of treatments that can be done for my case, but there are still all the other experimental approaches (the plan A’s) that are worth giving a shot. All this new stuff may not work, but in some people it has. In Dr. Wen’s opinion, I’m not limited to these standard treatments. In fact, there are several other treatments being developed that I did not mention in this post. It’s all uncharted, but I have hope.
In Limbo:
From my experience, the hardest part of developing a treatment plan is waiting. Waiting for scan results, blood work, genetic testing, etc.. It’s this disconcerting feeling of being in limbo. I want to do something to move the process forward, but there is nothing I can do. I know I have this tumor in my head that I want to start treating, but we need to wait to get all the results back to make a well-informed decision. In a situation where I already feel out of control, waiting amplifies my sense of powerlessness.
Despite this, I’m reassured knowing I have the captain I trust most to navigate me through these uncharted waters. While I have to wait until we get the genetic sequencing results back, I know Dr. Wen is putting everything in place so that we can start navigating our ship into the seas. A ship buoyed by the best science, knowledge, and medical artistry there is. Welded by the love and support of my family and friends.
Again, my intention isn’t to turn every post into a fundraiser, but hopefully the information I’ve shared with you epitomizes why funding for brain tumor research is so critical. Sunday, June 24th is the National Brain Tumor Society’s Bay Area Brain Tumor Walk where I will be the guest speaker. Please consider donating to, or better yet fundraising for, Team Jeremy so that these seas of treatment can become a bit more charted.

2 Replies to “Uncharted Waters: waiting for a treatment plan”