
Note: I would like to mention that all my medical results, doctors’ recommendations, and treatment decisions are my own personal experience. Everyone’s medical journey is unique. What I write is not an endorsement or recommendation for what anyone else should do. Rather, this blog serves as a window for my community, you, or someone you may know to get a glimpse into my experience living with brain cancer. Hopefully there are parts of my story that resonate, areas of connection particularly in the emotional aspects of cancer, that may be helpful to you. If you ever have questions related to what I write, please contact me.
Before I begin:
I apologize for the delay in writing a new post and responding to all your messages via this blog, email, and social media. Below is the reason why I have been rather preoccupied. I hope to respond to your messages as soon as I can.
The News:
September 25th, 11am: I sat in my doctor’s office at UCSF waiting for the results of my MRI. I’ve been in this same office numerous times with a picture of mountains hanging on its sterile white walls. Even as a medical student, I wonder why we design doctors’ offices this way. If you’re going to make it all white, keep it all white without putting up a picture of a place patients would rather be. Otherwise, and preferably, make the room more warm, welcoming…human.
But I digress. Let’s recap. After recovering from my surgery, I started an experimental treatment called Enasidenib, a treatment developed for Leukemia that has rarely been used for brain tumors. We hoped, based on my tumor’s molecular characteristic, that this drug would slow down or stop tumor growth. You can read more about the decision to do this treatment HERE. The seas of treatment were a little rough at first, but eventually things settled down, and the treatment became just another pill I took every evening. I was finally able to enjoy a couple months free from the ever-present thoughts of my illness. I started a new relationship, went back to school (part-time), and started writing as well as doing other fulfilling projects. It wasn’t sunshine every day; I continued to have focal seizures in my right arm about once a week, but I’d say the weather was mostly sunny with a touch of rain.
And then it was September 25th, 11am. Like all the other times before, my doctor came in and started asking how I’ve been feeling, what symptoms I’ve been experiencing, how was school, how was my relationship, etc., etc… At this point I was waiting for the scans. My doctor is filled only with good intentions, but she doesn’t have a good poker face. If she has good news, she’ll say it immediately when she walks in. If she doesn’t, she’ll converse for a bit before revealing the bad news.
With my Mom on speaker phone, my doctor said, “It’s not great news.” My stomach sank, and the sun that had shined for the past couple of months began to disappear. I immediately switched into expert-patient mode, trained with 15 years of experience and my Mom’s teachings. I asked for permission to record this conversation, and pulled out my phone app…on my phone’s screen, dates of past medical conversations spanning years.
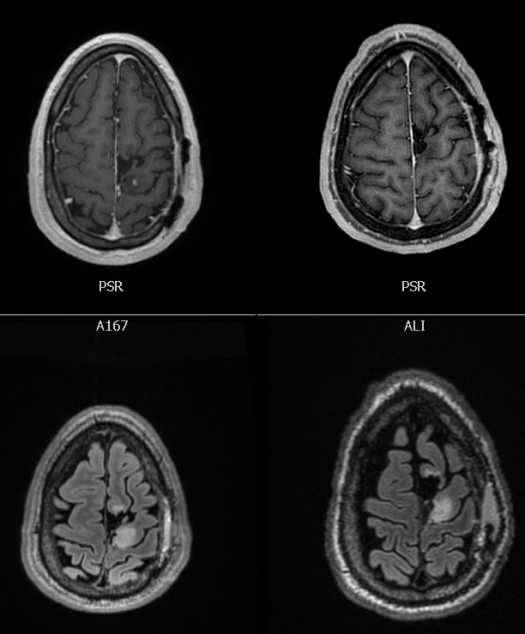
My doctor continued, “It looks like the tumor has grown. It looks denser, and in the image with contrast, there is a new spot appearing, indicating new growth.” She turned her computer screen and I looked at the MRI scans (seen below).
In these scans the brain is flipped. The tumor is in the left part of my brain (even though it appears on the right side of the image). The left side of the box are my scans from that September morning, and the right scans are from just two months prior. The top scans are images taken with contrast, which can show vascularization (new blood flow) of the tumor. If you look closely, the new scans show a little spot to the bottom-right of the resection cavity. New blood flow = tumor growth. The bottom scans show the tumor in white. The left is denser than the right, which also equates to tumor growth.
New tumor growth meant that the Enasidenib wasn’t working. It may have been fulfilling its biological role, but that alone was not enough to prevent my tumor from progressing.
My doctor shifted gears and began discussing treatment recommendations. She wanted to confer with UCSF’s tumor board, but felt that the next step was plan B from our past conversations: radiation and CCNU chemotherapy. It was the conventional approach with clinical evidence demonstrating its effectiveness. However, my tumor, with its molecular characteristics doesn’t fit into any of this research. As I’ve said before, I’m an N of 1. I was diagnosed with an adult tumor (an oligodendroglioma) as a kid. I’ve lived well-beyond the average life-span of those diagnosed with my type of tumor. I have rare mutation patterns (1p 19q co-deletion with IDH 2 but not IDH 1 mutation, unmethylated MGMT not methylated, and location in an area that’s inoperable). So yes, radiation and chemo is the most evidence-based conventional approach from large studies in Europe and Canada, but my tumor is not conventional.
Regardless, I thought this was my only option. With genetic results showing that my tumor was not hypermutated, I believed immunotherapy was off the table, and thus, radiation and chemotherapy were my next steps.
We scheduled an appointment with my radiation oncologist and set up the process to get insurance approval for the chemotherapy.
Brunch
For anyone who has read my past posts, you know that I have a go-to “Bad News Brunch” locale called Zazie. It also happens to be one of the best brunch spots in San Francisco, so I figure brain cancer is a pretty good excuse to spend the money on an omelet and home-fries that can help the sun shine through any cloudy day (I have yet to decide if I should leave a Yelp review). Eating with my friend, the only thing I could think about was not what was to come, but how I was going to tell my family and boyfriend.
The past two months had been spectacular, metaphorically and literally sunny each and every day. I was getting excited for my brother’s wedding and beginning a wonderful relationship with my boyfriend. During this time I often forgot about my tumor, but this tumor is always like a squall (a.k.a. storm) following me. Sometimes I can stay ahead, but every now and then it catches up. The news that the treatment hadn’t been working meant the squall caught up.
I didn’t want to bring this storm to my brother’s wedding or my relationship with my boyfriend. Doing this would be painful. Yes, my tumor is in my head, but my cancer impacts so many people around me. It may be in different ways, but the impact is no less difficult. When you love people, you don’t want to hurt them. I knew this news would be challenging. My love for my family and boyfriend pulled my heart away from wanting to hurt them with this cloud of cancer, but I knew I needed to be honest. I needed to tell them, so I did.
Consulting Yoda
While I was in Boston for my brother’s wedding, I met with Yoda (a.k.a. my doctor in Boston). Since he had not responded to any of the emails recommending radiation and chemotherapy, I expected he agreed with this treatment approach. Instead, he took out his lightsaber and made the treatment decision more complicated. Similar to our initial discussions following my surgery in May, my Boston doctor felt that chemotherapy would not be effective for my tumor.
Before I go on, I want to reiterate what my note says at the beginning of this post. Everyone’s tumor is unique; thus, everyone’s treatment options are unique. The details of my situation, and the treatments I’ve done and will do, should not determine what you as a reader should do. It is always better to collect more information from your healthcare professional, but I want to remind you that I am solely a 1.5 year medical student 😉
Now back to my story.
Rather than radiation and chemotherapy, Yoda felt radiation with immunotherapy might be a better approach. Why did he have a different opinion than UCSF? It comes down to one of the genetic aspects of my tumor called MGMT. As I’ve discussed in past blog posts, MGMT is similar to a repairman. If the tumor’s DNA is damaged, MGMT produces tools to help repair the DNA. Usually gliomas have methylated MGMTs, which essentially means that the repairman is asleep when chemotherapy attacks tumor DNA. Unfortunately, my MGMT is unmethylated, so my repairman never sleeps. He/She/They are always trying to fix my tumor DNA when/if chemotherapy attacks the tumor. Thus, Yoda doesn’t think chemotherapy will do much damage to my tumor.
In our meeting he was thinking of other ways we could attack the tumor. Usually, when you go to the doctor, you expect that doctor to come in with a game-plan like a football coach coming into the locker-room. My Boston doctor and I were trying to discuss and write-up the game-plan together, a testament to how my tumor does not fit into any standard therapy.
After some discussion, he recommended radiation combined with an immunotherapy called Pembrolizumab (also called Pembro). Pembro was developed for cancers in the body (not the brain); however, it has recently been used in trials for brain tumors. Unfortunately, Pembro alone has not had great success in treating brain cancer. Yoda; however, was not suggesting Pembro by itself. He wanted to try something that has never (to our knowledge) been tried before. He wanted to follow a hypothesis (explained below) called the abscopal effect, where the combination of radiation with Pembro could be more effective than both of those treatments alone. The literature and biological theory exists to support this approach, but the research has not yet been translated into clinical trials for brain tumors. Yoda, one of the most knowledgeable neuro-oncologists in the universe, explained that my case may fit the growing literature, but was too far ahead of the slowly developing research. We would have to try it before there was any clinical evidence.
He offered this approach as his opinion, and also mentioned that one of the determinants of my decision would rely on whether or not insurance would even cover the immunotherapy drug, Pembro.
Some Science and Goats (Immunotherapy)
If you would like to go down to my decision-making process and next steps, feel free to skip this section. Otherwise, I’ll try my best in a “concise” manner to explain how Pembro works from a medical student perspective as well as goat analogies.
Crazy Med Student Language (thanks to my classmates for some of this)
So, the goal of immunotherapy is to harness your body’s immune system to attack the tumor. Cancer cells are tricky because they have some strategies to protect themselves from the immune system. The figure below is from H. Dong’s chapter, The Basic Concepts in Cancer Immunology and Immunotherapy. Thanks Anthony! 🙂

As you can see in the figure, there is a tumor cell and a T cell. The tumor cell is cancer. The T cells are the soldiers of our immune system that try to fight off anything foreign in our body (including cancer). However, as shown in part A of the figure, tumor cells can have these things sticking out called PD-L1. When it attaches to its complimentary pair on the T cell, the T cell (the immune system soldier) is either put to sleep or sometimes killed. This is a problem because if all the immune system soldiers are sleeping then the tumor does not get attacked and can continue to grow.
This is one area where immunotherapy can save the day. In part B of the figure you can see some funny-looking triangular things called antibodies (name is not important) preventing PD-L1 from connecting to PD-1. Thus, the tumor can’t put the T cell immune system soldiers to sleep and they can attack the tumor. In addition to attacking the tumor, when these immune system soldiers attack, they can sound the alarm for reinforcements, and other T cells will come to help attack the tumor.
Pembro is called a PD-1 blocker. It essentially acts like the funny orange triangular things to prevent the tumor from putting the immune system (T cell) soldiers to sleep. Thus, Pembro keeps the immune system awake so that T cells can attack the tumor and call in more T cells to help out.
Goats (courtesy of Claire and Kelly)
For those who prefer goats, here is an analogy for immunotherapy: Imagine you have a lawn. In this lawn are some dandelions (cancer cells). Now there are a million goats (T cells of the immune system), constantly surveying this lawn. If a goat finds a dandelion (cancer cell) that it likes, it will reproduce a lot, so that they can all go hunt down even more dandelions. This is because one goat alone can’t mow an entire lawn of dandelions, but many very motivated ones can. Also, the goats that get rewards make copies of themselves.
However, some of these dandelions may have poisonous thorns (PD-L1) that make the goats sick. If the goats are sick, they can’t do their job to eat the dandelions, and they also can’t reproduce into a lot more goats. The dandelions keep growing.
Scientists, though, recognized this problem and developed special mouth-guards for the goats (Pembro) that protect them from the poisonous thorns. With this, the goats can eat the dandelions, and can also reproduce into more and more goats who can also eat the dandelions.
Hopefully, at some point you have a lawn free from dandelions (cancer) and full of goats (your wonderful immune system).
Harnessing the Abscopal Effect
Ready for some sci-fi?
Below is an image (from Wikipedia) demonstrating the Abscopal Effect. This is a hypothesis still under study that suggests radiation therapy can stimulate an immune response in the body, which can destroy tumor cells in another part of the body that did not receive radiation. (see figure below and ignore the words. Essentially radiation kills the red tumor cell, which then stimulates mini green boxes, our immune system, that travel through the blood to kill the orange tumor cell that did not get zapped by the radiation lightning bolt).

Unfortunately, it’s not that simple. If radiation could cure cancer in the whole body via the immune system then why is everyone with cancer not cured? Well, as I stated before in the immunotherapy section, tumor cells are smart and have many ways of evading our immune system.
However, scientists are now looking at the abscopal effect with a closer eye due to the advent of various types of immunotherapy. What if radiation can ramp up the immune system, and then immunotherapy can help the immune system kill more tumor cells? This potential teamwork scenario is what a lot of scientists are now looking into. The combination of radiation with immunotherapy may be able to harness the abscopal effect to enhance the effectiveness of both the individual treatments. Alone these treatments are okay, but together via abscopal, they may be great!
The evidence for this is growing, but there is very little clinical data, especially for brain tumors (i.e. the only glioma-related research I have found is on mice). The rationale makes sense, but does it translate clinically? No one knows…yet. It is very experimental.
For more scientific info on the Abscopal Effect you can read a recent NCBI article HERE
Making a Decision
I was presented with two opinions: radiation + chemotherapy or radiation + immunotherapy. There was no right or wrong answer. One opinion was based on evidence that I didn’t really fit into, while the other was based on research that I may fit into, but did not have a lot of evidence. One was conventional, the other was completely experimental.
I was overwhelmed.
I turned off my brain for my brother’s wedding so that I could be with my family, celebrate my brother and his wife, and savor in the moments that define what life is really all about.
After the wedding, I had to make a decision. In two months the tumor had grown, so we couldn’t wait too long. My doctors asked what my priorities were for treatment, but how could I know when there were no answers? The doctor’s had presented their opinions based on all the knowledge they had, and the decision was left in my hands.
In the end, the deciding factor could have been insurance. If they weren’t going to cover the immunotherapy, then I had no other option but chemotherapy.
I considered going to the National Institute of Health (NIH). I thought I could hear their thoughts. See what trials they had. Get a third set of eyes on the options I had been offered.
I didn’t go. It would have taken several weeks to see someone…time I didn’t have, and I already had two of the top institutions helping guide me through this decision.
To make a decision, I needed to get all my thoughts organized. I went back through the meetings I had with my doctors (…each one recorded), and came up with a list of questions. I talked with my doctor in Boston, which led to more questions for my doctor at UCSF. After my call with UCSF, I had more questions for my doctor in Boston, so I talked with him again.
At this point I had all the information, but still no easy choice. I needed to make a decision without answers.
I chose radiation with immunotherapy.
Why? Mostly gut…with a splash of logistics and a tiny bit of safety net.
I’ve had a long relationship with Yoda, so I think that figured into my decision. However, as a patient, I never follow with blind faith. I needed him to thoroughly explain his reasoning for his treatment opinion. With that understanding, and knowing that UCSF would be willing to administer the immunotherapy (an immense privilege of coordination that few people have access to) , I had to go with my gut.
Additionally, my gut had a safety net. If the radiation and immunotherapy combination does not work, then I still have the option to do chemotherapy. On the other hand, if I did chemotherapy first and it impacted my immune system, then that would lower my chances for effective immunotherapy down the road.
Next Steps
I made my decision, and waited to see if insurance would come through.
It did! But only for Dana Farber since Yoda originally applied for it.
I sent an email to my care team informing them of my decision. I asked UCSF if they could apply for insurance coverage, and made sure everyone was on the same page.
As of publishing this post, I found out on Friday, October 19th that insurance will cover immunotherapy at UCSF. Once I received this news, the floodgates opened, and within the span of twenty-five minutes, I received four phone calls from UCSF and several emails scheduling an MRI, immunotherapy, and radiation. October 24th is my first immunotherapy infusion, which will continue every three weeks for the foreseeable future. October 25th is my first of ten continuous days of radiation treatments.
None of this may work. I may have side effects (expected and unexpected), especially since this is my second time doing radiation. We’ll never know, but perhaps chemotherapy may have been the better route.
It’s all unknown.
In the world of uncertainty all I can do is make as much of an informed decision as possible, hope, and in the meantime hold onto everything that brings presence and love into my life.
With love,
Jeremy
A slight note: I’d be amiss if I did not acknowledge the plethora of people supporting me. I am truly privileged to have access to the best medical minds there are. As someone studying medicine for the underserved this is always an ever-present reality I must acknowledge and call out. I’m grateful to my medical team, family, boyfriend, friends, and greater community for their support in guiding me through this journey.

Dear Jeremy, You are fighting a good fight. I am praying for you with all my heart and soul!!
Carol Roblin.
LikeLike
Fear Jeremy o was a friend of your grandfather ron. He would be so proud of you. All my best to you and my prayers.
LikeLike